His-Purkinje System

When electrical activity has been slowed in the AV node, it
enters a very rapidly conducting set of specialized conducting tissue, the
His-Purkinje system. The bundle of His is the initial portion and is a fairly
thick bundle of cells. Its electrical activity routinely shows up on an
appropriately done intracardiac electrophysiologic evaluation (but not on the
surface ECG), as the His spike (Fig. A). Isolated heart block in this
particular anatomic structure is relatively uncommon. When it occurs it is
categorized as infranodal block and is a potentially dangerous form of heart
block. The bundle of His almost immediately splits into components of the
Purkinje system. These are the left and right bundles. The left bundle is
divided into the left anterior and left posterior fascicles (thus the term
trifascicular block for infranodal complete heart block). Disruption of these bundles is quite common and left
bundle branch block (LBBB) and right bundle branch block (RBBB) are routinely
diagnosed on EKGs. The clinical significance of this block is dependent on the
clinical scenario and can range from completely benign to pathologic as
discussed below.
Figure A His Bundle Recording.

A: The normal His bundle recording demonstrates an A
deflection corresponding to the P wave on the surface ECG. The H deflection
occurs during the isoelectric period between the P wave and the QRS complex and
is due to activation of the Bundle of His. The V deflection corresponds to the
QRS complex. B: Prolonged AH interval (>140 msec) block within the AV node.
C: Prolonged HV interval (>55 msec) block below the AV node.
Nomenclature of AV Block
Mobitz type I block is characterized by gradual lengthening
of the PR interval in sequential beats until there is a nonconducted P wave
(Fig. B). One important way to identify this is to look for a difference in
the PR interval of the beats preceding and following the dropped beat. With
Mobitz I second-degree AV block, the AV node has had time to recover after the
dropped beat and the PR interval will be shortest after the dropped beat,
compared to all other PR intervals. This type of block usually occurs in the AV
node and the native QRS complex is narrow, unless there is coincidental bundle
branch block present. The term Mobitz I block can be a description of block in
other parts of the conduction system. For our purposes, we will assume the more
common occurrence, block in the AV node.
Figure B Nodal Versus Infranodal Heart Block.
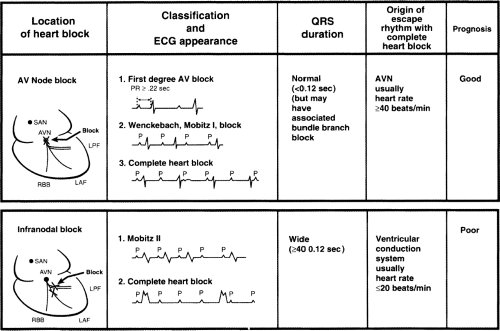
A statistically and clinically significant association
between ECG pattern and the anatomic location of block is shown. In general,
block within the AV node is often benign (with some important exceptions), and
block of second or third degree below the AV node has a more consistently poor
prognosis. The less common situation of Mobitz I second-degree AV block in
association with a wide QRS complex is not depicted in the figure. This type of
block can be caused by nodal or infranodal block and may require investigation
with electrophysiologic studies. Rarely the Mobitz II second-degree AV block
can occur with a narrow QRS complex due to block in the His-bundle itself,
without associated BBB. (SAN, sinoatrial node; AVN, atrioventricular node; RBB,
right bundle branch; LPF, left posterior fascicle; LAF, left anterior
fascicle.)
Mobitz type II second-degree AV block is described as a
dropped P wave, but with no progressive lengthening of the PR interval before
the dropped P wave and no difference in the PR interval before or after the
dropped beat (Fig. B) . This type of block occurs almost exclusively in the
His bundle or the Purkinje system. Block in the isolated His bundle is quite
rare. If this did occur, then the subsequent QRS could be narrow. The much more
typical situation is block in the Purkinje system and this is usually
associated with wide QRS complex. A logical way to view this is that it is
unlikely that all three major branches of the Purkinje system (right bundle,
left anterior fascicle, and left posterior fascicle) would conduct
simultaneously and then block simultaneously. Almost always two of the three
fascicles are “broken” or not conducting, leading to a wide QRS complex and the
third fascicle conducting intermittently.
In around 75% of cases, the conduction block is located
distal to the Bundle of His, producing broad QRS complexes.
In the remaining 25% of cases, the conduction block is
located within the His Bundle itself, producing narrow QRS complexes.
It is of note that patients with 2:1 block, ventricular
conduction with every other P wave, cannot be categorized into Mobitz I or
Mobitz II block simply because you cannot tell if there is prolongation of the
PR. On the other hand, a long rhythm strip will often locate consecutively
conducted beats and clarify the type of block.
Third-degree AV block, also known as complete heart block,
describes the failure of any depolarizations to pass from the atria through the
AV node and His-Purkinje system to the ventricle. The atria may beat regularly
in response to the SA node (or the patient could be in atrial fibrillation).
The ventricles beat independently in response to whatever intrinsic rhythm has
taken over: the AV node, the His bundle (junctional rhythm), the Purkinje
system, or cells in the ventricle. The escape rate below the AV node may be
about 50 bpm with junctional rhythm (although this may be highly variable) or 0
to 40 bpm in the ventricle with a ventricular escape rhythm. Third-degree AV
block is a potentially dangerous rhythm, depending on the clinical setting. For
example, third-degree AV block can occur in the setting of an acute inferior
wall myocardial infarction (MI) with block in the AV node and an adequate
junctional rhythm. This is virtually always a transient event. If the heart
rate is unduly slow, a temporary pacemaker is required. There are clinical
situations in which observation is adequate with standby transcutaneous
pacemaker and immediate availability of atropine to speed up conduction through
the AV node, if required. This would be a relatively benign form of
third-degree AV block. On the other hand, third-degree AV block due to chronic
degenerative disease of the His-Purkinje system can lead to syncope or sudden
cardiac death.
Blood Supply of Conducting System


Rate of escape rhythm from various areas of the conducting system.
Electrogram of
Much of our understanding of the conduction anatomy of the
heart has come from study of the intracardiac electrogram, often referred to as
the His bundle electrogram. Depolarization of the AV node and the His bundle
produces no deflection on the surface ECG; however, a closely spaced bipolar
electrode can be positioned across the anterosuperior portion of the septal
tricuspid valve leaflet, in close proximity to the His bundle. A depolarization
spike originating from the common His bundle can be recorded (refer to the H
spike in Fig. A). On the intracardiac ECG, atrial (A) depolarization precedes
the H spike, and ventricular (V) depolarization follows the H spike. The
interval between the atrial and His depolarizations (AH interval) reflects
conduction through the AV node. The HV interval is the result of conduction in
the Purkinje system between the His bundle and the ventricles. Thus, AH
interval prolongation indicates a conduction abnormality within the AV node
(above the His bundle), and HV interval prolongation indicates an infranodal
conduction abnormality in the Purkinje system (left and/or right bundle). A
potential value of measuring the His bundle electrogram is to document an
abnormally long HV interval. An interval of greater than 100 msec, implies a
significantly diseased Purkinje system that, in the presence of worrisome
symptoms, may even warrant pacing. Pacing the atrium rapidly with the
development of infranodal block can also be an indication of a significantly
diseased His-Purkinje system.

