Basic concepts
THE ATRIOVENTRICULAR DELAY
The AV delay determines the longest time interval between an atrial event and the programmed delivery of a ventricular pacing pulse. This interval is the electronic equivalent of the PR interval.
The programming of the AV delay intends to ensure optimal mechanical coordination between atrial and ventricular contractions, whether the atrium is sensed or paced. The length of these intervals can be programmed within a wide, fixed or adaptable range and influenced by a large number of algorithms.
Paced AV delay
A paced AV delay is implemented after atrial pacing when the pacemaker operates in DDD, DDI, DVI and DOO modes.
The observed duration of the paced AV delay might differ from the programmed value because of interactions with the following algorithms:
- Adaptable AV delay
- AV delay+ hysteresis
- Ventricular safety pacing
- Non-competitive atrial pacing
Sensed AV delay
The sensed AV delay is implemented after a sensed atrial event when the pacemaker functions in atrial synchronized pacing mode (DDD and VDD).
The observed length of the sensed AV delay might differ from the programed value because of interactions with the following algorithms:
- Adaptable AV delay
- Automatic PVARP
- AV delay+ hysteresis
- Wenckebach function of the pacemaker during exercise
Setting of the AV delay
The optimal AV delay varies considerably among patients.
The precise programming of the AV delay must allow the maintenance of a constant temporal relationship between left atrium and ventricle and ensure that the left atrial systole has just ended at the onset of left ventricular systole.
The permanent programming of long AV delays to promote spontaneous conduction in patients who are pacemaker non-dependent can now be avoided by implementing the MVP mode. Indeed, a programmed AV delay that is excessively long can be associated with: 1) an enhanced risk of pacemaker-mediated tachycardia (PMT), 2) an enhanced risk of pacing during the vulnerable period of an ventricular extrasystole that was not sensed because it fell during the post-atrial ventricular blanking after atrial pacing, and 3) an adverse hemodynamic effect with fusion of the E and A waves, premature closure of the mitral valve, and valvular regurgitation due to the reopening of the valves at the end of the ventricular diastole.
An inappropriately short programmed AV delay can be associated with 1) a borderline atrial ejection volume with a loss of the active component, and 2) valvular regurgitation in early systole.
If the patient is pacemaker-dependent (complete AV block), the mean value of the optimal, sensed AV delay at rest approaches 110 ms.
Paced versus sensed AV delay
The optimal sensed AV delay is shorter than the optimal paced AV delay for several reasons:
- instead of being sensed at the very onset of the surface P wave, the P wave is sensed at the passage of the atrial depolarization signal under the electrode, which is often delayed with respect of the onset of the P wave on the surface ECG.
- when the P wave is paced, the electro-mechanical delay is longer than when the P wave is of sinus origin; the conduction time between right and left atria is prolonged.
- the difference between sensed and paced AV delays depends on the position of the lead in the right atrium: on average this difference is 30 ms if the lead is in the inter-atrial septum, 50 ms if it is in the appendage, 70 ms if in the high lateral wall, and ≥90 ms if in a low lateral position. These average differences, which must be evaluated and adapted to each individual, are often longer in presence of intra- or interatrial conduction disorders.
- this difference changes minimally with exercise, though tends to shorten under the influence of catecholamines, which shorten interatrial conduction. In presence of major interatrial conduction abnormality, this difference can increase during exercise. Typically, however, this value may remain unchanged within the entire range of programmed changes in rate.
Adaptable AV delay
The PR interval normally shortens with exercise. The adaptation of the AV delay as the heart rate increases is intended to mimic this physiologic phenomenon; the same adaptation is imposed on the sensed and paced AV delay.
The specific characteristics of the adaptable AV delay will be presented in the chapter discussing the settings during exercise.
REFRACTORY PERIODS OF SINGLE CHAMBER PACEMAKERS
The refractory period is an interval following a paced or sensed event in the chamber containing the pacing or sensing lead, during which the inhibited (SSI) or triggered (SST) pacemaker is not reset. In a VVI pacemaker, the first part of the refractory period is a programmable, absolutely refractory blanking period. It prevents the resetting of the pacemaker by the sensing of a) post-pacing ventricular potentials, b) the end of the QRS, or c) the T wave. The occurrence of an event during the blanking period is not visible on the marker channels.
The programmed duration of the refractory period is usually between 220 and 350 ms.
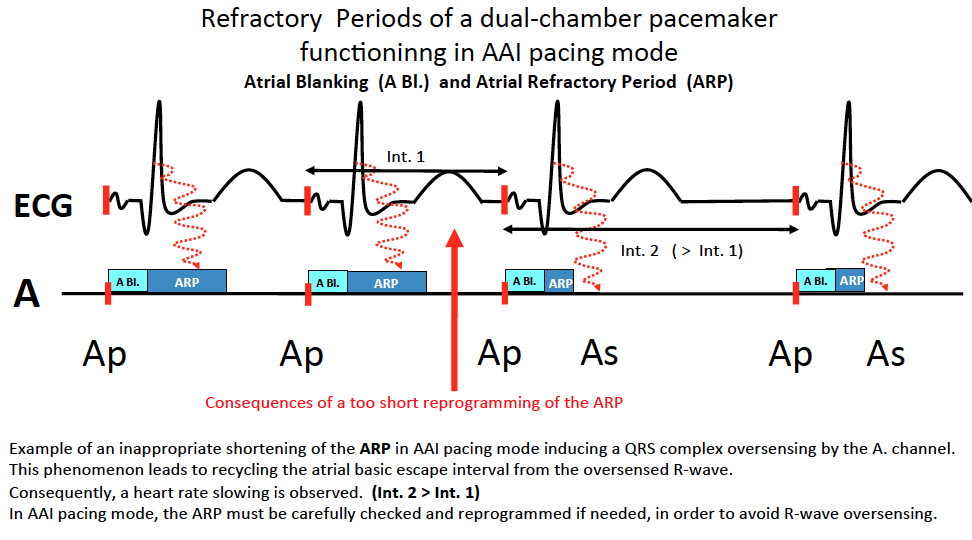
The programming of an excessively short refractory period facilitates oversensing, which is reflected by a resetting of the escape interval and a slowing of the pacing rate. The programming of an excessively long refractory period incurs a risk of non-sensing of ventricular premature events. In that case, a stimulus might be delivered at the end of the pacing interval on the T wave of the extrasystole. In AAI pacemakers, the first part of the refractory period is a programmable blanking period. The refractory period prevents the resetting by an R wave sensed in the atrium (ventriculoatrial cross talk). Its duration must be as long as the AR interval (between the atrial stimulus and the R wave), which is longer than the PR interval, though not inordinately long to ensure atrial sensing up to the maximum sensor-driven rate.
REFRACTORY PERIODS OF DUAL CHAMBER PACEMAKERS
Atrial or ventricular pacing initiates different blanking and refractory periods in the paced chamber as well as in alternate chambers in order to prevent cross talk.
Two types of refractory periods are implemented in DDD mode:
- The blanking periods completely deactivate sensing for a programmable or nonprogrammable interval to protect against:
- post-pacing potentials in each chamber;
- atrioventricular or ventriculoatrial crosstalk;
- Longer refractory periods, during which sensed events are included in the diagnosis of arrhythmias and in the proper function of various algorithms. In contrast, a spontaneous event sensed during a refractory period does not reset the synchronization interval.
The refractory periods prevent the resetting of the pacemaker by unwanted signals such as retrograde P waves or electrical interference.
It is noteworthy that in new pacemaker models, the differentiation between a) blanking (absence of sensing and inscription of the signal on the marker chain) and b) refractory period (preserved sensing and presence on the marker chain) is less clear-cut. Thus, an event sensed during blanking might be visible on the marker chain and interfere with the function of various algorithms.

Post atrial pacing ventricular blanking
This programmable ventricular blanking period, triggered by an atrial stimulus, prevents sensing of that stimulus by the ventricle, which would inhibit ventricular pacing and cause ventricular asystole in a pacemaker-dependent patient presenting with complete AV block.
In the event of a ventricular extrasystole occurring during the post-atrial pacing ventricular blanking, a risk is incurred of ventricular pacing during the vulnerable period. This blanking period is usually programmed between 30 and 40 ms

The safety window
The safety window is a ventricular sensing period that complements the post-atrial ventricular blanking. It is implemented only after atrial pacing. The sensing of a ventricular event after the post-atrial ventricular blanking triggers a ventricular pulse at the end of this safety window. In case of ventricular extrasystole, the pulse is triggered during its refractory period. In case it has sensed an artifact or a late atrial stimulus, ventricular asystole is prevented.
This function is available when the pulse generator operates in DDD, DDI and DVI modes.
The duration of the safety window is 110 ms, or is identical to the paced AV delay if the latter is <110 ms. A short AV delay on the ECG indicates the occurrence of pacing in the safety window. While ventricular safety pacing can be programmed ON or OFF, it is advised to systematically program it ON. The annotations VS and VP are visible on the real-time monitor tracing, on the “frozen” tracings and on the printed tracings.

The blanking period and the post-ventricular ventricular refractory period
All events sensed or paced in the ventricle trigger a non-programmable ventricular blanking period, the duration of which is dynamically modulated by the pacemaker according to the amplitude and duration of the ventricular stimulus. The dynamic blanking prevents the repetitive sensing of a same event.
The ventricular refractory period (VRP) occurring after a sensed or paced ventricular event prevents sensing of the T wave. A ventricular event sensed during the VRP does not recycle the pacemaker.

Atrial blanking and atrial post-atrial refractory period
The atrial blanking and atrial refractory period (ARP) follow paced or sensed atrial events.
The blanking period and the ARP are used in the AAI or AAT modes.
If the pacemaker is programmed in MVP mode and functions in AAI mode, the ARP is automatically adjusted to 75% of the cardiac cycle, up to a maximum of 600 ms.
The blanking period and the ARP are used in the AAI or AAT modes.
If the pacemaker is programmed in MVP mode and functions in AAI mode, the ARP is automatically adjusted to 75% of the cardiac cycle, up to a maximum of 600 ms.
Post-ventricular atrial blanking
It is typically an absolute refractory period enforced in the atrium after ventricular sensing and pacing. The PVAB represents the beginning of the PVARP.
Its role is to prevent the sensing by the atrial chain :
- of the ventricular pacing stimulus
- of the spontaneous or paced QRS.
It operates in DDD, DDI, VDD and VDI modes.

The post-ventricular atrial refractory period
The post-ventricular atrial refractory period (PVARP) is triggered by ventricular sensing or pacing and is implemented in DDD, DDI and VDD modes.
Its main role is to prevent the sensing of retrograde P wave that might trigger a pacemaker mediated tachycardia in the P wave synchronous modes. When the pacemaker is in DDI mode, the PVARP prevents the atrial inhibition by sensing of retrograde P waves.
Its initial component is occupied by the PVAB, which was traditionally the absolutely refractory. Beyond the PVAB, the period is relatively refractory. During the PVARP, intrinsic atrial events might be sensed and identified as refractory (AR) on the event marker channel, though its does not modify the synchronization of the pacing intervals. Thus, an atrial event sensed during this period does not initiate an AV delay. When the pacemaker is in DDD or DDI modes, the expected atrial pacing is not inhibited.
In order to prevent the resetting of ventricular pacing by a retrograde P wave, the PVARP must be programmed at a value longer than the ventriculoatrial conduction time of the patient. The mean retrograde conduction time is between 220 and 280 ms, though might be longer, which requires an adaptation of the PVARP in each individual patient.
An excessively long PVARP might cause the development of 2:1 block during rapid sinus rhythm, when the pacemaker operates in P wave synchronous mode (DDD or VDD). To increase the 2:1 point, the PVARP may be configured to vary as a function of the sensor-indicated rate (sensor-modulated PVARP) or by the mean atrial rate (automatic PVARP). The details of the exercise-dependent settings will be reviewed in another chapter.
While they cannot reset the synchronization interval, the events sensed during the PVARP are used by the pacemaker toward functions that require a knowledge of their periodicity or frequency (mode switch, response to ventricular extrasystoles, adaptable AV delay, automatic PVARP and NCAP). The sensed refractory events are included in the telemetry of the event markers.



PROTECTION AGAINTS PACEMAKER-MEDIATED TACHYCARDIAS
Onset, duration and rate of pacemaker-mediated tachycardia
The onset of a PMT requires:
- the programming of a P wave synchronous mode (DDD or VDD)
- intact retrograde conduction loss of AV synchronization; a properly synchronized ventricular and atrial activity blocks
- retrograde conduction.
Retrograde conduction is present on average in 40% of unselected patients who are paced at rest(up to 80% prevalence in patients paced for sinus node dysfunction, considerably higher than in patients paced for AV block). During exercise, the mean prevalence of retrograde conduction is 75%. This high prevalence justifies an effective protection, which should be systematically programmed.
The following events might promote AV dissociation, retrograde conduction and the onset of PMT:
- a ventricular extrasystole (the most frequent cause);
- an atrial extrasystole with lengthening of the AV delay to respect the programmed upper rate;
- an excessively long programmed AV delay; the nodo-hisian tissue has recovered its excitability at the time of ventricular pacing;
- an external interference or myopotentials sensed by the atrial chain;
- an atrial sensing or pacing defect;
- absence of PVARP extension after removal of a magnet, or exit from fallback upon 1:1 AV re-association;
- application and removal of magnet;
- VDD mode programming in a patient in sinus rhythm at a rate slower than the programmed back-up rate;
PMT is a repetitive sequence in which the pacemaker responds to each retrograde P wave by pacing the ventricle at a rapid rate, which, in turn, produces a retrograde P wave. This cycle repeats itself indefinitely unless interrupted by retrograde block or by the intervention of a specific pacemaker algorithm.
A long-lasting PMT may be poorly tolerated, with symptoms ranging from ill feeling or palpitations to cardiac decompensation in patients suffering from underlying heart disease.
The rate of PMT depends on:
- the retrograde conduction time,
- the programmed upper rate,
- the existing AV delay.
If the retrograde conduction time + the AV delay (at the upper rate) is shorter than the shortest pacing cycle (60,000/upper rate), the rate of the PMT is equal to the programmed upper rate, the AV delay being prolonged with each cycle.
If the retrograde conduction time + the AV delay (at the rate of the PMT) is longer than the shortest pacing cycle (60,000/upper rate), the rate of the PMT is slower than the programmed upper rate and equal to 60,000/(retrograde conduction time + AV delay), and the AV delay is that programmed at the ongoing rate. This hypothesis is observed in approximately 35% of cases.
Prevention of onset of pacemaker-mediated tachycardia
Several measures can help prevent PMT, including:
- the programming of a mode such as DDI which prevents the onset of PMT. It is a pacing mode, which might not be suitable for some patients (absence of ventricular pacing synchronized with sensed P waves).
- the programming of a PVARP longer than the retrograde conduction time, which can be measured at the time of implantation. One must keep in mind, however, that the programming ofan excessively long PVARP might cause intolerable 2: 1 AV block during exercise. The programming of a PVARP, or adaptable AV delay, or both, can increase the exercise capacity. A PVARP programmed at 300 ms prevents the development of PMT in a majority of patients.
- avoidance of all instances that might promote a loss of AV synchrony.
- programming of short instead of long AV delays
- program a sufficient safety margin to ensure proper and permanent sensing and pacing
- program bipolar atrial sensing to prevent the sensing of myopotentials or outside interferences
- automatically lengthen the PVARP upon magnet removal
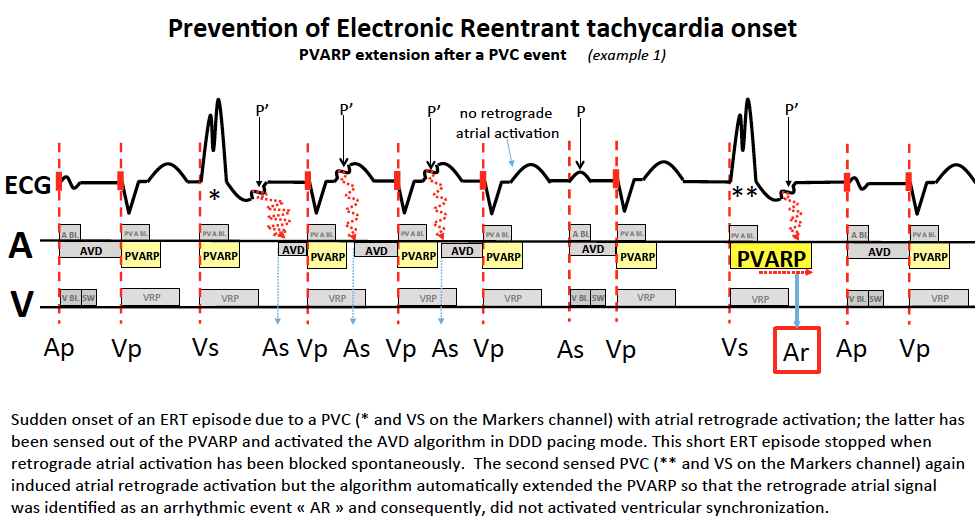
- the response to premature ventricular complexes (PVC) prevents the tracking of retrograde P waves originating from PVC. The pacemaker defines PVC as any sensed ventricular event that follows another paced, refractory or sensed ventricular event in absence of interim atrial event. When the PVC response is ON, a PVC initiates a 400-ms PVARP if its programmed value or the on-going value is <400 ms.
Diagnosis of pacemaker-mediated tachycardia by the pacemaker
Diagnosis of pacemaker-mediated tachycardia by the pacemaker The anti-PMT intervention is available when the device functions in DDD, VDD, or MVP mode. With MVP mode, the anti-PMT intervention functions only in DDD mode.
The pacemaker diagnoses a PMT when it detects 8 consecutive VA intervals which fulfill all these
conditions:
The pacemaker diagnoses a PMT when it detects 8 consecutive VA intervals which fulfill all these
conditions:
- VA interval <400 ms
- VA interval begins with a paced ventricular event
- VA interval ends with a sensed atrial event
Using the activity sensor-indicated rate, the pacemaker verifies that the eight consecutive VA intervals are tracked retrograde P waves instead of an intrinsic accelerated atrial rhythm.
- if the sensor-indicated rate is below or equal to the ADL rate, an episode of PMT as defined by the device is confirmed and therapy is delivered.
- if the sensor-indicated rate is > than the ADL rate, rapid sinus rhythm is diagnosed and no therapy is delivered, and,
- the pacemaker continues its monitoring of series of eight consecutive VA intervals along with the sensor-indicated rate.
Anti-pacemaker-mediated tachycardia therapy
This algorithm interrupts PMT by lengthening the PVARP and sensing the next retrograde atrial event in the refractory period. This refractory event does not synchronize ventricular pacing and the tachycardia is interrupted.
When a PMT is detected, a 400 ms PVARP is introduced after the 9th paced ventricular event. If a PMT is ongoing, the extended PVARP ensures that the next sensed atrial event occurring within a 400 ms delay will be refractory.
Sinus tachycardia might prompt an anti-PMT intervention, causing a single P wave during the PVARP, consequently not tracked by the pacemaker.
When a PMT is detected, a 400 ms PVARP is introduced after the 9th paced ventricular event. If a PMT is ongoing, the extended PVARP ensures that the next sensed atrial event occurring within a 400 ms delay will be refractory.
Sinus tachycardia might prompt an anti-PMT intervention, causing a single P wave during the PVARP, consequently not tracked by the pacemaker.

Following an intervention, the anti-PMT function is suspended automatically for 90 sec, preventing repetitive and unnecessary interventions in cases of rapid and stable intrinsic atrial rates.
The anti-PMT intervention function interacts with other pacemaker functions:
- atrial non-competitive pacing (NCAP) is automatically activated for one cycle after the 9th ventricular paced event of a PMT episode. The function NCAP can shorten the next paced AV delay to stabilize the ventricular rate.
- if mode switch is programmed ON, the anti- PMT intervention is temporarily deactivated in case the pacemaker switches to the atrial non-tracking mode. It is reactivated as soon as it has returned to atrial tracking.


No comments:
Post a Comment